UPPER GASTROINTESTINAL SUBEPITHELIAL TUMORS
.jpg)
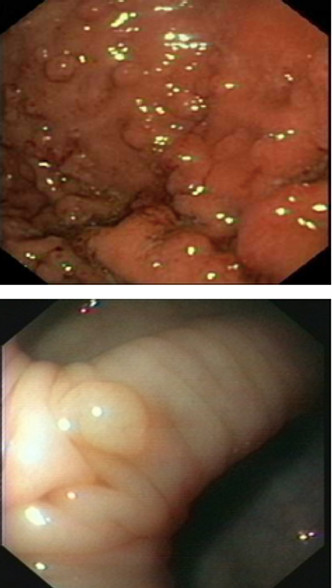
Gastric gastrointestinal stromal tumor (GIST) with rapid growing. (A) Endoscopy didn’t detect any mass in the stomach. (B) Four years later, endoscopy showed round smooth elevated mass in gastric angle. (C, D) Enodoscopic subtumorial resection was performed. Tumor size was 1.7 cm
• Most lesions are asymptomatic and clinically insignificant
• GIST is the most common subepithelial tumor to occur in the stomach
• The risk of GIST metastasis cannot be accurately predicted before lesions are completely resected
• Most of these are benign. Endoscopy and EUS are helpful to distinguish malignant tumors
NON-HODGKIN’S LYMPHOMA

Induration of the gastric wall and multiple deep ulcerations are always suspicious for malignancy. Left image: malignant infiltration of the gastric folds; Middle image: ulcerated malignant mass; Right image: malignant infiltration of the pylorus
Malignant tumors of the stomach account for only 5% or less of all malignant neoplasm in chil- dren. The most common malignant gastric tumors in children are non-Hodgkin or Burkitt’s lym- phoma or gastric involvement in lymphoprolifera- tive disorder after solid organs or bone marrow transplantation

Burkitt’s lymphoma of the stomach and the small intestine. Loose teeth were the presenting symptom. EGD was performed to evaluate progressive weight loss, abdominal pain and anemia. Multiple erythematous nodules with or without ulcerations and infiltration of the gastric wall were found. The diagnosis was confirmed morphologically of the gastric and bone marrow biopsies. Left picture: multiple ulcerated masses in the proximal stomach; Middle picture: ulcerated masses along the greater curvature of the stomach; Right picture: focal malignant infiltration of the duodenum
GASTRIC ADENOMATOSIS
• Gastric adenomas are common in patients with FAP (familial adenomatous polyposis) and can be difficult to identify endoscopically
• Endoscopists should have a high degree of suspicion for gastric adenomas in these patients and a low threshold to biopsy
• Malignant foci was confirmed by endoscopic biopsy
• Given the benign clinical course, recommended initial management is conservative with endoscopic therapy and periodic surveillance.
Surgery should be reserved for patients with adenomas having advanced histologic features who fail endoscopic manageme
Related posts
- Forrest classification for ugib - 03-05-2021
- Dieulafoy’s lesion - 29-04-2021
- Henoch-schonlein purpura - 04-05-2021
- Crohn’s desease - 03-05-2021
- Pertrophic pyloric stenosis (hps) - 03-05-2021
- Lymphangiectasia (lae) - 03-05-2021
- Celiac sprue - 04-05-2021
- Lymphoproliferative - 03-05-2021
- Gastric foreign bodies - 03-05-2021
- Gastric polyp - 04-05-2021
-

Self-design suction tool
20-05-2021 -

Removing phytobenzoar in Pig's stomach
20-05-2021 -

Remove twisting of the pig colon
04-05-2021 -

Pig stomach endoscopy
04-05-2021
-

Management of Ingested Foreign Bodies in Children: A Clinical Report of the NASPGHAN Endoscopy Committee
28-04-2021 -

Management of Familial Adenomatous Polyposis in Children and Adolescents: Position Paper From the ESPGHAN Polyposis Working Group
28-04-2021 -

Pediatric Colonoscopic Polypectomy Technique
28-04-2021 -

Gastrostomy Placement in Children: Percutaneous Endoscopic Gastrostomy or Laparoscopic Gastrostomy?
28-04-2021







