ENDOSCOPIC GASTRITIS: SYDNEY SYSTEM
1.Endoscopic erythematous/exudative gastritis
2.Endoscopic flat erosive gastritis
3.Endoscopic raised erosive gastritis
4.Endoscopic atrophic gastritis
5.Endoscopic haemorrhagic gastritis
6.Endoscopic rugal hyperplastic gastritis
7.Endoscopic enterogastric reflux gastritis
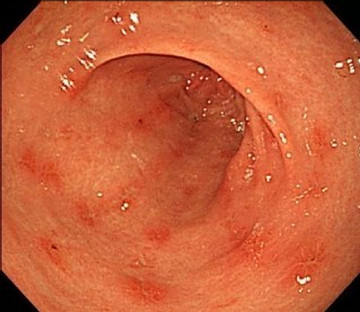
1. ERYTHEMATOUS/EXUDATIVE GASTRITIS
.jpg)
• Gastric mucosal loss of gloss, slightly lumpy, with each congestion, bleeding easily when touching. The mucosa is red strip more markedly than adjacent mucosa.
• Erythema of gastric mucosa is either diffuse, focal or linear
2. FLAT EROSIVE GASTRITIS
•Superficial lesions limited to mucosal lining
•Linear or aphthoid
•Typically white or yellowish base surrounded by a narrow zone of erythema
•May be multiple and vary in size
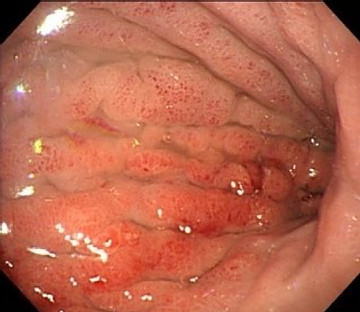
3. RAISED EROSIVE GASTRITIS
.jpg)

•Elevated, inflamed border surrounding a small depressed central necrotic patch
•The center may be hemorrhagic, or yellowish
•About 5 – 10 mm
•They appear as a series of nodules or bulges on the crests of the folds
4. ATROPHIC GASTRITIS
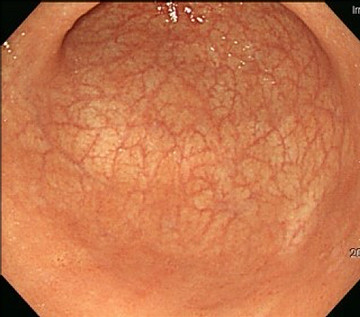

•Folds of gastric mucosal are disappear or
5. HAEMORRHAGIC GASTRITIS
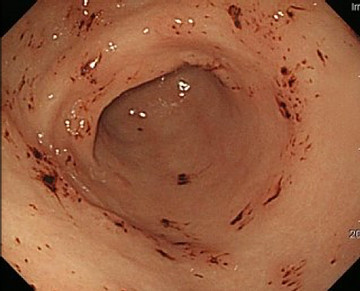

•Mucosal or submucosal hemorrhagic spots are predominant
•These spots are reddish or brownish black, of variable size, and usually sharply delineated
•It should be differentiated from gastric purpura due to thrombocytopenia
6. RUGAL HYPERPLASTIC GASTRITIS

•Gastric folds are considered enlarged when the folds are larger than 5mm
•Giant folds that do not flatten during maximum insufflation suggest an inflammatory or infiltrative process
•The surface may be erythematous, erosive, exudative
•Large caliber forceps is recommended to take a sufficient deep
7. ENTEROGASTRIC REFLUX GASTRITIS
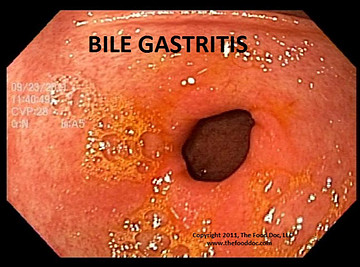

•Gastric mucosa is edema, congestion, hypertrophy and bile in the stomach
•Characterized by abdominal pain, bilious vomiting, and weight loss
•Antacids, cholestyramine
•Consider surgery
INITIAL MANAGEMENT
•Check the patient’s medical history for infection, stress, radiation, allergies, food poisoning, or trauma, using of compounds including NSAIDs, steroid, and aspirin
•Biopsy 3 sample at antrum, body, angle for urease test, histological, culture HP
•Treatment:
•Change life style and eating habits, stop or reduce the dose of drugs that affect the stomach
•Use antacid
•Confirm the presence of Helicobacter pylori and treatment based on protocol
Related posts
- Forrest classification for ugib - 03-05-2021
- Dieulafoy’s lesion - 29-04-2021
- Henoch-schonlein purpura - 04-05-2021
- Crohn’s desease - 03-05-2021
- Pertrophic pyloric stenosis (hps) - 03-05-2021
- Lymphangiectasia (lae) - 03-05-2021
- Celiac sprue - 04-05-2021
- Lymphoproliferative - 03-05-2021
- Gastric Tumors - 03-05-2021
- Gastric foreign bodies - 03-05-2021
-

Self-design suction tool
20-05-2021 -

Removing phytobenzoar in Pig's stomach
20-05-2021 -

Remove twisting of the pig colon
04-05-2021 -

Pig stomach endoscopy
04-05-2021
-

Management of Ingested Foreign Bodies in Children: A Clinical Report of the NASPGHAN Endoscopy Committee
28-04-2021 -

Management of Familial Adenomatous Polyposis in Children and Adolescents: Position Paper From the ESPGHAN Polyposis Working Group
28-04-2021 -

Pediatric Colonoscopic Polypectomy Technique
28-04-2021 -

Gastrostomy Placement in Children: Percutaneous Endoscopic Gastrostomy or Laparoscopic Gastrostomy?
28-04-2021







